

Written by Dr Allada – 11 March 2023
Lidia Perin Medical Centre – Suite 1, 12 Napier Close DEAKIN ACT 2600
Ph (02) 6162 1886 Fax (02) 6162 1887
Like many other medical practitioners, I have become increasing aware that the biggest drug addiction in the Western world is to something most people would think is harmless. Yet this seemingly innocuous substance causes major health problems and as a result is a huge burden to our healthcare system.
Whilst we all know about societal problems associated with alcohol, tobacco, and illicit drugs such as heroin or cocaine, carbohydrate addiction causes much greater adverse health effects than these drugs and substances combined. We were told 70 years ago, on the basis of some very dubious research, that fat was the cause of heart disease, the so-called ‘diet-heart hypothesis’. The food industry responded by producing a wide range of low-fat, highly processed, and ultra-processed foods. Unfortunately, when manufacturers removed fat from food, it affected the taste, so sugar was substituted. This change in eating habits became mainstream with the 1980 release of the Dietary Guidelines for Americans, which discouraged the eating of saturated fat and cholesterol. This low-fat, high-carbohydrate dietary recommendation persists to this day across the globe, including in our Australian Dietary Guidelines. The Australian Dietary Guidelines were last released in 2013 but there is another release scheduled in 2024. We have had a low-fat, high-sugar diet for 40 years, yet we have gotten fatter and sicker ever since.
In 2001 Walter Willett, Professor of Epidemiology and Nutrition at Harvard T.H. Chan School of Public Health, published ‘Eat, Drink and Be Healthy: The Harvard Medical School Guide to Healthy Eating’ after observing that a substantial decline in dietary fat consumption was associated with a very large increase in the level of obesity. This problem remains an ongoing issue with two thirds of Australian being overweight or obese. Sadly, a quarter of Australian children are overweight or obese. Cardiovascular diseases such as heart attack and stroke have soared. Since 2000 Type 2 diabetes has seen a four-fold increase globally and affects 8% of Australian adults.
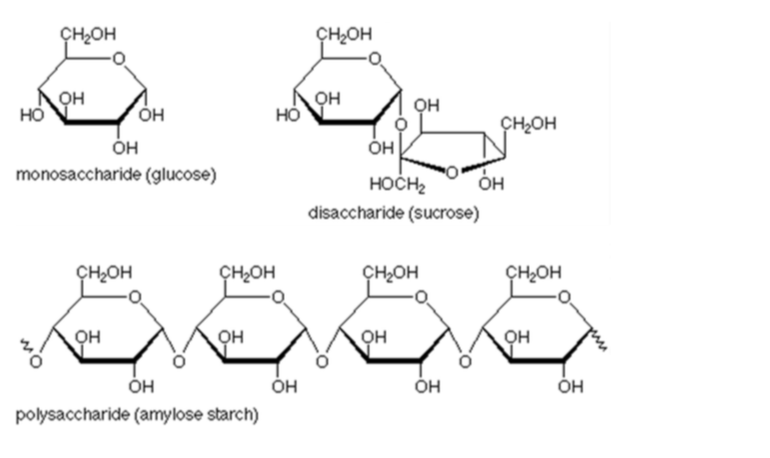
There are three types of carbohydrates:
- Simple carbohydrates (monosaccharides and disaccharides) release sugar quickly into the blood, raising our blood sugar level. They are found in honey, dried fruits, grapes, syrups and nectar, table sugar or sucrose, coconut sugar, milk, soft drinks, sweet biscuits, cakes, chocolate, and confectionary.
- Complex carbohydrates are absorbed more slowly than simple carbohydrates, but they still impact your blood sugar levels. Complex carbohydrates are found in bread, pasta, rice, cereals, couscous, quinoa, millets, starchy vegetables, and fruit. Starchy vegetables include beans, squash, chickpeas, corn, lentils, parsnips, peas, potatoes, sweet potatoes, taro, and yams. Fruits with the highest carbohydrate content include grapes, banana, mango, cherry, and pineapple.
- Dietary fibre moves slowly through the digestive system. In humans very little fibre is digested, so it has no impact on our blood sugar level. It can be found in certain fruits, vegetables, and wholegrains. Fruits high in fibre include passionfruit, avocado, guava, and raspberries. It is well established that fibre is important as part of a healthy, balanced diet because it promotes good bowel health and reduces constipation and bowel cancer. It is not recommended to fully eliminate carbohydrates from our diet and in particular fibre due to its positive effects on bowel health. That is why the CSIRO Low-carbohydrate diet includes a limited amount of high-quality, high fibre, low glycaemic index (low-GI) carbohydrate foods to ensure that our diet meets daily fibre recommendations.
I am often asked what a low-carbohydrate diet is. A common definition is as follows:
- Very low (‘ketogenic’): 20-50g/day
- Low: <130g/day
- Moderate: Between 130-230g/day
- High: >230g/day
Table sugar (sucrose) is made of equal parts of fructose and glucose. Fructose gives sugary products like fruit their sweet taste. Glucose is the other component and results in most of our problems. As soon as glucose is absorbed from our gut into the blood stream, it triggers the release of the hormone insulin from the pancreas. Insulin helps move glucose into our cells, where it is either stored as glycogen in our liver and muscle or used immediately as an energy source. When glycogen stores are full, the excess sugar is converted to fat. With prolonged and excessive consumption of sugar, the cells in our body fill with glucose. The insulin level rises to push more glucose into our cells, but a point is reached when insulin cannot push any more in. We now become insulin resistant. This results in type 2 diabetes. It is thought that persistently elevated blood glucose levels cause many of the complications of type 2 diabetes such as blindness, kidney disease, amputations, cardiovascular disease, and dementia. More than 23,000 Australian deaths in 2021 were attributable to diabetes. The annual cost of diabetes to the Australia’s health system is estimated to be $20 billion.
Pure alcohol is not strictly a carbohydrate but rather is a sugar that has been fermented. It therefore still contains a lot of energy. On a per 1000g basis fat provides 37,656 kJ, pure alcohol provides 29,288 kJ and protein and carbohydrate provide 16,736 kJ. As there are no other nutrients in alcohol it is often described as ‘empty calories’. Many alcoholic beverages do however have additional carbohydrates.
The amount of carbohydrate in 1000 g of the following common alcoholic beverages can be seen below:
- spirits (rum, vodka, gin, tequila, scotch, whiskey): 1.0 g
- low-carb beers: 5.0 – 14 g
- light beers: 24 g
- mid strength beers: 14 g
- full strength and dark beers: 30 g
- alcohol free beers: 70 g
- non-alcoholic wine: 40 g
- white wine: 19 – 35 g
- red wine: 24 – 37 g
- dessert wine: 140 g
We are all different and each of us have a craving to different things that contribute to us being overweight. Some people drink too much beer or wine, others love fruit, yet others eat too much bread or rice. It is important we look at our diet and identify what our food weaknesses are and thereby address these areas. In 2020 I saw a female patient that used to be 150kg. Her mother at her deathbed pleaded with her to better look after her health. At this stage my patient could only walk 5 m before becoming short of breath. Despite these limitations she heeded her mother’s advice and created three rules around food: 1. ‘What she could eat?’ 2. ‘How much she could eat?’ 3. ‘When could she eat?’. With these simple rules she lost 48 kg in 14 months. She was now able to walk 3 km. I was very impressed with her fortitude and when she left my office, I said to her: ‘14 months ago you lost your mother. Look at my practice manager. She is 48kg. You have lost her too.’
Our bodies are not designed to consume large amounts of carbohydrates. There was only a small amount of carbohydrate in our diets 100,000 years ago and for the hunters and gatherers then it was only seasonally available. Unlike fat and protein, which are essential for many of our body tissue structures and functions, the main role of carbohydrate is as a quick energy source. However, when there is insufficient energy from sugar or glycogen, we do not ‘run out’ of energy. Instead, our body uses protein and fat for energy. Whilst we have receptors for protein and fat to tell us when we have had enough, there are no such receptors for carbohydrate. When we eat meals containing predominantly protein or fat, we develop a sense of fullness. That is protein and fat in a low carbohydrate eating program reduce the feeling of hunger. Although more difficult you can still put on weight if your protein and fat intake is higher than energy expenditure.
Notwithstanding the positive benefits of fibre on gut health, there is no carbohydrate, including any grain, that is essential in a human diet. You cannot survive on zero protein or zero fat, but you can survive on zero carbohydrate. You may not be happy with no sugar and carbohydrate in your diet, but you will survive.
Refined carbohydrates are long chain of sugars which break down to single glucose molecules in the gut. There is not a single biochemical process in our bodies that demands we ingest sugar or carbohydrates. And yet, they are the major ingredients of most packaged ultra-processed foods. Carbohydrates make you hungry. They quickly result in an increase in your blood glucose level, and then your blood glucose level drops right down again. Two to three hours later you are hungry again. We should therefore avoid eating meals which have a significant carbohydrate load. This then leads to us overeating and therefore to us becoming overweight.
One problem many people have is not being able to distinguish between true hunger and cravings for sweet foods. Sugar is as addictive as nicotine. It triggers the reward centre in our brain, releasing neurotransmitters such as dopamine, which makes us feel good and therefore crave more. That is why we often consume sugary foods to feel better when we are down or anxious. Our brain needs to balance the stress hormone cortisol by releasing ‘feel-good’ chemicals and sugar is effective at triggering this. This is not helped by sugar being relatively cheap. As sugar is omnipresent, we are constantly being tempted. Knowing this, modern food scientists produce foods as desirable as possible by having their ratios of sugar, fat and salt precisely crafted for maximal palatability (and addiction). This is said to be the ‘bliss point’ and is why modern processed foods can be hard to resist. Many of my general practitioner colleagues tell their patients and themselves ‘this is poison’ every time they ingest sugar or carbohydrate.
There are animal studies in rats which demonstrate that sugar is more addictive than cocaine. In one study, mice in one group were fed and became addicted to sugar, and in the other group they were fed and became addicted to cocaine. These substances were then withdrawn from each of the groups and the mice’s brains were analysed to determine the effect of withdrawal of these substances. The brains of the mice withdrawn from sugar lit up greater than those withdrawn from cocaine. This indicates greater withdrawal effects from sugar compared to cocaine.
Unfortunately, giving in to our cravings only reinforces our addiction. To identify cravings, try the ‘cheese test’. If you think you are hungry, ask yourself if you would eat cheese, or another non-sweet low carbohydrate food. If you are just craving, and not truly hungry, you are likely to say no.
Withdrawal effects from sugar include difficultly concentrating, fatigue, dizziness and light-headedness, headache, being jittery, intense cravings for sweet things, irritability, nausea anxiety, changes in sleep pattern, and depressed mood,. These withdrawal effects share many similar characteristics to withdrawal from nicotine or narcotic drugs. It is therefore important to remember when you experience these feelings your blood sugar level is not low. Instead, you are having a withdrawal from sugar. You can only develop hypoglycaemia, a low blood glucose level if you are diabetic and are on insulin or are taking diabetic medications that drop your blood glucose level. A person without diabetes cannot develop hypoglycaemia even with prolonged fasting unless they have an insulin producing tumour of the pancreas which has an incidence of less than 1 person per million adults per year. If you are overweight, you have fat stores, and these stores can be broken down to provide energy and therefore keep your body functioning.
When you walk into a supermarket, there are two places that tend to catch your eye: the checkout (where unhealthy items are eight times more likely to be discounted than healthy food items) and the end of isle displays. Here, unhealthy food like chocolate and confectionary, chips and unhealthy drinks are strategically placed to capture your attention. These junk foods are officially known as ultra-processed food and beverages. Examples of these foods are breakfast cereals, frozen meals, sweet biscuits, soups, sauces and dressings, processed meat and seafood, fast food, cakes, ice-cream, frozen dessert, and salty snacks. They include drinks too, like sports and energy drinks, soft drinks, juice drinks and nectars and ready-to-drink tea and coffee. They have almost no nutritional value, yet they are given prime position. A similar thing could be said about many of our politicians.
In October 2017, for six days prior to my birthday, I did not eat breakfast or lunch but only had dinner. I consumed only water during the day. Although I was hungry especially towards the end of the day, I was able to function normally. This included patient consultations, performing complex procedures in hospital and some would say more importantly being a chauffeur to my children. I wanted to go longer than 6 days but was persuaded to partake in the beautiful birthday lunch prepared for me. I did not lose any weight over this time, and this presumably was because I consumed my daily requirement in the evening. What however was interesting was that after a few days I developed a higher level of concentration and was able to work with less breaks despite this period of fasting. Since that time, I have done several fasts greater than 40 hours. To illustrate this, I ate dinner late on Sunday night with my next meal being Tuesday’s dinner. For me, the difficult times were trying to sleep on an empty stomach on Monday as well as late Tuesday afternoon. Again, I drunk plenty of water and have used my busy life to distract me. When I felt mentally weak, I used ‘the inspiration in my life’ to encourage me. I have been able to function at a high level during these periods of fasting. I call this period of fasting ‘skipping 5 meals’ and this has made it easier for me to miss one or two meals.
I routinely now do not eat breakfast. It is a fallacy to say that ‘breakfast is the most important meal of the day’. Whilst this statement may hold some validity for growing children it is not true in adults, especially overweight adults. There is now evidence to suggest people who routinely skip breakfast weigh less than those who eat breakfast.
I however have seen greater loss in weight in patients that do not eat after a certain time in the evening, for example after 6 pm. I believe weight loss here is because we are often mentally weaker at the end of the day. This then results in us eating much more than we should. Sometimes after a long and mentally arduous day at work I feel like Dr Jekyll and Mr Hyde. I do not feel particularly hungry when I get into my car, nor whilst I am driving the short distance home but as soon as I enter the front door, I turn from Dr Jekyll into Mr Hyde.
In another animal study, one group of mice were overfed and not surprisingly became overweight, and the other group were given usual amounts of food. They then starved the overweight mice and as predicted these mice returned to their previous weight. They then allowed both groups of mice to eat as they pleased and the group that initially became overweight became overweight again. I remember a female patient lamenting that her ‘body shape’ before her first pregnancy was that of a ‘lollipop’ and she was never able to regain her pre-pregnancy weight or size. I also remember my accountant relating to me that he was considered ‘low weight’ as a child. His mother took him to a doctor who prescribed high dose steroids. His appetite improved as did his weight. Unfortunately, his weight kept increasing till at a weight of 169 kg he required bariatric surgery.
Therefore, anyone who is overweight or who has been overweight has to accept that they are a sugar (carbohydrate) addict and therefore must be careful with their intake and types of food they eat for the rest of their life. It is very hard to lose weight. In fact, you will have to try harder than someone with a drug addiction to lose weight. Once you have lost the excess weight, your battle has only just begun because as soon as you ‘take your eye off the ball’ your excess weight will usually return.
I have spoken to a few patients that have never been overweight and have realised there is a difference between them and people such as myself who have been or who are overweight. The difference is people who have never been overweight are not obsessed by food, they forget to eat unless they are reminded to do so. If they are very stressed, they almost stop eating. If such people were stuck in a room alone filled with a variety of delicious foods and an interesting book, they would read the book with little distraction, eating only when they had to and eating only the amount they needed to.
We have three options in how we consume our meals. Firstly, we can eat until we are full and feel sick. I do not recommend this as when I have eaten excessively, as I am sure many of us have at times, I feel very uncomfortable and regret what I have just done. Secondly, we can eat until we feel content but no more. This sounds logical, but it should be remembered that there is a time lag between when our stomach is full and when our brain registers this. As a result, we eat slightly more than we should. The third and correct option is to continue to have the feeling that we want to eat more when we end our meal. I recommend this as I believe it teaches us to restrict our intake and therefore assists us in losing weight. We need to learn how to deal with hunger which is key to weight loss.
It is important that we teach our mind (some would say our tongue) to rely less on sugar as it stimulates our appetite. Water is the best drink and should be the drink of choice for anyone that is overweight. Often patients try and substitute sugar in their diet with artificial sweeteners which have no calories. Some use artificial sweeteners in their coffee and some bake with it. I used to drink Pepsi Max or Diet Coke. We feel happy because there are no calories, yet the food or beverage tastes sweet. There is however a ‘catch’. When we taste something sweet, our brain assumes that sugar will follow. When this does not occur our brain ‘feels tricked’ and compensates by eating more. Likewise, when you take your child into a toy store, and they want a toy you may initially placate them by saying you will buy the toy later. But when you walk past this toy on the way out of the store your child remembers your promise and if you do not buy it, you then need to manage a ‘meltdown’. There is evidence that people who consume artificial sweeteners put on weight rather than lose weight. I have now tried therefore to avoid consuming drinks with sugar or artificial sweeteners. If I now want a fizzy drink, I will have sparkling mineral water. To get a little taste I sometimes add one drop of dōTERRA essential oil into a 600 ml bottle of water or sparkling mineral water. The essential oils that I like include grapefruit, lemon, and wild orange. Alternatively, you can cut a thin slice of citrus fruit and place this into the water bottle.
Overweight patients often ask me how much weight they should lose. I attended a cardiology conference 10 years ago and the presenter stated, ‘We should be able to wear the same pants we did when we were 20 years old’. When a lady in the audience asked ‘What about us? We have had children. Does the same rule apply to us?’ the reply from the presenter did not change.
In my opinion, our ideal weight is that where there is little or no fat on our body. For men they should have little or no fat on their abdomen and for women they should have little or no fat on their bottom. The reason I say this is because this is the last place in general fat leaves a man or a woman. The ‘mirror test’ is therefore the best test in the morning to remind you whether you need to lose weight. For many patients this seems an impossible task, but weight loss should be taken slowly. If people who are overweight burn slightly more energy in the day than what they consume they will be successful in achieving weight loss. I ask my patients to try and achieve 1.0 kg of weight loss per month. For a very overweight person, the desired weight loss may take many years. Remember ‘Rome was not built in a day’. On taking our dog, Blaze, to a routine visit to the vet we were given the following advice, ‘if you can feel the ribs on him then he has a good weight’. I realised this was not just good advice for Blaze but also for us.
I have had patients who successfully lost weight say their young grandchildren take time to adjust to them as they look different and are no longer as cuddly. Several years ago, I had a patient that recently lost 32 kg of weight. He had attended his nephew’s wedding and the patient’s brother made enquiries as to who the ‘wedding crasher’ was. When he was told that it was his own brother he was astounded and immediately greeted his sibling. People are often asked if they have cancer because of their significant weight loss. It is better however to look like you have cancer but feel well rather than to feel like you have got cancer because you are so overweight but ‘look good’.
Anyone who has lost a significant amount of weight has excess skin. When you blow up a balloon and it is then deflated it never looks the same as a new balloon. But remember, it is more important how you feel rather than how you look or what others say. People who have lost a significant amount of weight move around much more easily, have less shortness of breath, and have a better quality of life. These people are happy and proud, as they should be, of their achievement.
Poor people in third world countries have a very low weight not out of choice but because they have no choice but to work very hard with very little food. Such people often only get one small meal per day, remain hungry at the end of their meal, and fill their stomach with water to try and overcome their hunger. I frequently tell my patients: ‘you may live like a king or queen, but you should eat like a pauper’. That means eating simple food and only eating the amount that is necessary. Two other keys things I tell my patients to try and lose weight are ‘to not eat when you are not hungry’, that is do not eat because someone asks you to or because of circumstances, and ‘when you are hungry to try and eat less’. My biggest temptation in overeating often occurs at home in the evening. I therefore tell my patients that if their pantry is full, it is harder to lose weight. Very poor people also open their pantry in the evening but as it is empty, they then close the door and go to bed. One patient jokingly said her pantry was stocked better that Coles. She was very obese. Some of my patients try and give up sweets but replace them with large servings of fruits. Remember eating too much fruit (or worse still fruit juice) means consuming large amounts of sugar. It is important to note that fruit is nature’s candy.
When patients come back for review and have put on rather than lost weight they say ‘We tried to exercise more. Why did I put on weight?’ As dietary restriction is very difficult, it is understandable that they have been unsuccessful as they tried ‘only a little bit’ to lose weight instead of trying harder than someone with a drug addiction.
Dieticians frequently note that patients routinely underestimate how much they eat and overestimate how much exercise they do. I often use the ‘car’ as an example to illustrate this point. It takes 2 minutes to fill a car fuel tank, but you can drive this car for up to 8-10 hours before the tank is empty again. The same analogy applies to eating and exercising.
Sometimes patients compare themselves to another person who is not overweight and compared to them they exercise and eat the same amount. They are upset therefore as to the discrepancy in their weights and state that it is unfair. I remind them that eating the same amount as a lower weight person may not result in either person losing weight. For the overweight person to lose weight they need to eat less and exercise more than the lower weight person. That is, they need to create a deficit of energy intake over expenditure. Once they become the same weight they can then eat and exercise the same amount as the other person.
There are now many phone applications to help you record exactly how much you consume and accurately record how much exercise you do. Often people struggling with their finances keep a budget of all their income and expenses. This assists them in budgeting. Likewise, phone applications that give a record of our energy intake and expenditure also help us to successfully budget our food intake and activity expenditure. They help us identify areas of high calories consumption and allow us to make informed decisions on which unhealthy food habits we need to target.
Patients often ask, ‘How long do I need to diet for?’, I remind them that a diet is often for a specific purpose, for example, to lose weight to attend your daughter’s wedding, after which you may return to your former size. More importantly to be successful long term in losing weight you need to make a lifestyle change that you can commit to for the rest of your life. This is the only way to achieve long lasting weight loss. There are no magic medications or remedies to lose weight. But there is a multibillion-dollar industry (increasing from USD 246.8 billion in 2022 to USD 405.4 billion in 2030) falsely promising easy weight loss.
To some extent, weight loss is about learning to manage our feeling of hunger and trying to conquer the feeling that we should eat when we are stressed. Weight loss is about learning to make do with less. To lose weight you are in effect temporarily and slowly starving yourself. I remind patients that poor people do not get the opportunity to eat excessively just because it is their birthday, or it is Christmas. What they eat for the day depends on what they have earnt for the day. If they do not work for the day, they get to eat very little. I inform my patients that their income is not what is in their wallet but what they physically do each day. A poor person who is not able to find work for the day is equivalent to us when we are on holiday lying on the beach sipping cocktails or travelling on a long-haul flight. Our intake likewise needs to be adjusted to these situations. If we keep telling ourselves, we will eat what we want today because we will burn it off tomorrow, we are doomed to fail. The sad reality for most of us is ‘tomorrow never comes’.
It is important to take responsibility for your weight loss. One of my long-standing patients in the past underwent gastric sleeve surgery when she was 330 kg and with this her weight reduced to under 100 kg. Her weight then started to increase and in 2021 when I reviewed her, she was 130 kg. She was scheduled to have a second bariatric procedure, namely gastric bypass surgery. Despite spending $36,000 on the second operation, she only lost 9 kg of weight. Her general practitioner had a stern talking with her and instructed her to take responsibility for her weight. My patient therefore hired a personal trainer, exercised regularly and significantly reduced her caloric intake. It was these changes, not bariatric surgery, that resulted in her reducing her dropping her weight to 80 kg. I was very proud of her determination and mental strength and have no doubt that her goal to lose a further 12 kg will be achieved. Her aim is to reduce her weight to that before she tragically lost her husband which is what first led to her weight to spiral out of control.
I am often asked the question with regards to whether low-fat milk is better than full-cream milk. I give the example of Pauls Smarter Milk which has half the fat of full-cream milk but more calories than full-cream milk. This is ‘not smart’ and is typical of low-fat milks that have more calories than you would expect. The best and cheapest way to create low-fat milk is to add water to full-cream milk.
My weight was 66 kg, at the age of 18, when I started medicine at the University of Melbourne in 1991. By 2006 I was mildly obese. I had just moved from Ballarat to Canberra to commence an interventional cardiology fellowship. On my first day at work and whilst in the change room with an interventional cardiologist I was told not to use the standard scrubs as they would be too small for me. One the same day one of the nurses in the cardiac catheterisation laboratory looked at my stomach and jokingly said I was pregnant. I then decided that things needed to change with my weight. I bought a cross trainer and a treadmill, and I did a huge amount of exercise over a period of five months. My diet was similar although I did seem to eat less in the evening. I lost 21 kg and dropped my weight from 84 kg to 63 kg. I recall an entertaining incident following my weight loss. In November 2005 shortly before starting my interventional cardiology fellowship I reviewed a patient. His wife was also in attendance. In February 2006 he saw a locum cardiologist in Ballarat as I was in Canberra that day. I then reviewed the patient in August 2006 and both he and his wife seemed very grumpy. After 10 minutes I paused the consultation and asked why they were both so grumpy. The wife of the patient replied, ‘Last year we saw Dr Allada. In February this year we had to see a locum cardiologist as Dr Allada was away. Now we must see you!’ I replied, ‘I am Dr Allada!’. They broke into smiles, and the consultation resumed without the grumpiness.
I could not drop my weight below 63 kg and when I exercised more, I found that I became prone to respiratory tract infections. Life got busier again and my weight slowly increased to 71 kg by 2016. Each time I told a patient to lose weight I was also telling myself, so it was very frustrating to me personally that I could not succeed. I became determined to again lose weight when I was correctly told that I was overweight, and more importantly this was because I was eating too much. This statement was my inspiration to lose weight. I became determined that I needed to apply all the principles I had been telling my patients to myself. I saw a photo of myself when I was 63kg and said I want to again be that person.
In November 2016 I conducted a weight loss experiment on myself. I wanted to see how much weight I could lose in one week with exercise. From a baseline of 1-2 hours of exercise a week I did a big week of exercise which included 270 km on my mountain bike, 250 km on my road bike and an 8 km jog. This equated to 24 hours exercise for the week. During this time, I roughly consumed the same amount of food. My biggest temptation was white rice, so I switched to roti (flat Indian bread) which I did not like as much and therefore ate less. After 1 week of this extreme amount of exercise I had lost only 0.7 kg. Although disappointed, I was not surprised as it is said that you need to run for 152 km at a speed for 10km/hr to burn 1 kg of fat. As an aside, uranium provides on a weight-to-weight basis 2 million times more power than fossil fuels. Fat is therefore the uranium of energy storage in our body.
Despite the initial lack of weight loss, I kept exercising intensely although not as much as I had done in the first week. I exercised for a total of 27 days consecutively where I did at least 2 hours of exercise per day. This equated to 1300 km on my bike and 6 half marathons. After this time, I had lost a total of 2.5 kg. Following this period, I was not able to exercise as much because of work commitments but became stricter with my diet. To my surprise although I was only able to exercise on 3 occasions over the next subsequent 2 weeks, I was able to lose a further 3 kg. Sitting inactive burns about 300 g of fat per day. Sadly ‘my most successful weight loss stories’ are very frail, elderly patients who never leave their house. Why? Because they no longer have any appetite. These patients lose 5-10 kg of weight per year in their last years of life. For the rest of us we struggle with weight loss because when we are strong our appetites are equally as strong. The best way to lose weight is to eat less, not exercise more. It is important to understand that most of our energy expenditure is used to keep us alive with only a small additional amount expended for exercise. Therefore, if you meditated all day and consumed very little food you would lose more weight than if you exercised to an extreme but ate more.
In addition to white rice my other addiction is to milk chocolate. In late 2016, I purchased a block of 99% dark chocolate. After six months I finally finished the 100g block. In October 2017, I gave up chocolate for one month. Prior to making this decision, I had tried unsuccessfully to reduce my chocolate intake despite getting family members to hide the chocolate in the house. During this month of abstinence, chocolate was not hidden. It was very liberating to be able to see chocolate and not eat it. Whilst it was an amazing experience to celebrate with chocolate after 1 month, I now knew that I was in control of chocolate and that chocolate was not in control of me. Although I still enjoy rice and especially chocolate, but I have learnt I can live without them. Many women who become pregnant make a commitment to their unborn child and modify their dietary habits. They stop alcohol, do not eat soft cheeses, sushi, or pâté, do not consume raw eggs, soft serve ice-cream and avoid cold meats. If they were smoking prior to their pregnancy, they stop. If women can make these sacrifices for their unborn child, we can also make dietary changes for our health.
I conducted another experiment on myself. It occurred between two Christmas parties in 2016. There was a coronary care unit Christmas party which I attended to on Thursday evening. I ate and like most of the people there, regrettably consumed more than I needed to. The next morning, I performed a procedure in the private hospital and then undertook procedures at the public hospital. I did not eat breakfast as I was not hungry. At lunchtime, although starting to become hungry, I decided to not eat for that day. I did this for a personal reason, but I also wanted to test my will power. As soon as I made this commitment, the cardiac device representative announced that he was bringing a beautiful Thai lunch for all the staff. I knew this was my first temptation but told him ‘Thank you for your gesture and I am sure the staff will enjoy this lunch, but I will not be eating. I will however sit with you all.’ He asked what I would like, and I told him that I would like sparkling mineral water. I watched my fellow staff eat and could smell the beautiful aroma of the food. I was also tempted each time I went to the coronary care unit as during this festive season there was chocolate everywhere. I opened the chocolate box, smelt the aroma, however I did not eat any chocolate.
Once I finished work at the public hospital, I then had to attend to two sick patients in the private hospital. There were further food temptations that evening but I was able to resist. I arrived home at 11.30pm. It had been a very long day as I had started work at 6.45am. I was pleased with myself that I was able to get though the day and perform all my duties without eating. I was able to concentrate fully despite many complex procedures. All I had consumed during the day was water. On Saturday morning I did a bike ride with my group. There is no doubt that I had by then depleted my glycogen stores and was not as strong, but I was still able to cycle the usual 50 km. After this bike ride, we all attended a fellow cardiologist’s house for Christmas breakfast. The bread-and-butter pudding tasted like it was ‘made in heaven’. I had succeeded in fasting for 36 hours.
The healthiest people who live into their 90s and 100s aren’t people like me that try and use exercise to keep their weight down. The healthiest people are active people that do not go overboard with their exercise yet are able to keep their weight stable with a simple diet. I now tell my patients that the most important muscles to use to control weight are the muscles that close our mouth. To say no to delicious food is very difficult but it is so important if we want to be successful in losing weight.
Data suggests that those that do not exercise at all are more likely to die because of health problems. Interestingly the lowest mortality rate is amongst people that are active without going overboard with their exercise. That is the lowest mortality is in people that do the equivalent of 2.5-5.0 hours of brisk exercise per week. Those that exercise more than 10 hours per week have an attenuated longevity benefit. This is called the Reverse J-Curve for Exercise. Those that push themselves to extremes when they are older yet continue to eat badly not surprisingly have a relatively high incidence of vascular events including heart attacks and strokes. When explaining sensible exercise to my patients I use the analogy of a car. I state that when we buy a new car we can ‘floor it’ without any problem. When the car is old however there can be problems if we ‘floor it’. The key to a long life is a simple diet as this keeps your weight low without having to resort to extreme exercise. Exercise should be enjoyed and not used as a tool to lose weight. Although pushing yourself during exercise can be fun, I usually tell my patients to exercise to level that if they were to be rung on their mobile phone that would find it difficult to maintain a conversation without slowing down.
Given the fact that sugar is more addictive than cocaine, does it not follow that we are doomed to fail in our quest to lose weight. This is not necessarily the case. It is important to understand how hard the task is and create a plan to succeed. It is important to find yourself an inspiration to succeed or determine an important reason why you want to lose weight as this is what you will need to think about when things get hard. Of course, you may have occasional, for me it has been frequent, relapses but the longer you fight the more likely you will eventually succeed.
In the two months leading up to an Italian bike ride holiday in September 2017 I trained very hard. This included 26 hours and 530km in one week on a mountain bike. My weight only dropped from 63.5kg to 62.5kg with two months of intense training because I ate sufficiently for the exercise I was doing. In Italy I rode a road bike consecutively for ten days with a total distance of 850km and this included 13.4km of vertical ascent. I put on 1kg despite this huge amount of exercise because I ate and drank too much. As I have said it is very easy to eat more than any amount of exercise that you can do. That is, ‘you can’t out train-a bad diet’.
Upon returning to Australia later that month, I again exercised the most important muscle to lose weight, that is the ‘muscles that close my mouth’. I now was too busy to exercise as I have had to dedicate a lot of my time to our clinic’s amazing new redevelopment. Despite not exercising as much, I dropped my weight to 61kg in January 2018. I was then encouraged in the six weeks before Easter to try a vegan diet. I realised by adopting a vegan diet that there were so many foods that I liked and could not have. It was a very good lesson in self-control. With a vegan diet, I was able to reduce my weight to 57.8 kg on the 14th of April 2018. I was very proud of myself as I had lost a total of 26kg from my peak weight in 2006, 13kg from my weight in late 2016, and 5kg less than the person I again wanted to be at 63kg.
My long-term aim is to use food abstinence intermittently and to keep my weight below 63 kg. With the vegan diet, I have realised that the bigger the selection choice in food you have, the higher is your weight. Eating vegan food itself does not make you lose weight especially if you find vegan alternatives, such vegan burgers, vegan pizza, or vegan cakes. These vegan alternatives often have more calories than their non vegan equivalent. Reduced choice in food options leads to reduced weight. I have accepted that weight loss is therefore 90% diet and only 10% exercise. Obviously, the goal is to be like the lower weight person who has access to all food but only eats the amount that is required. This however may an impossible goal for many people including myself. Those who have conquered their obsession of food are truly amazing people.
It is very important that our dietary intake changes and that we significantly reduce our carbohydrate intake. We need to focus more on meat and fish, non-starchy vegetables, and low sugar fruits such as berries, eggs, full-fat dairy, and nuts such as pistachio and walnuts. Low carbohydrate diets are enjoyable, sustainable, nutritionally rich and avoid hunger and calorie counting. It is important we are active without going overboard with exercise. It is essential that we incorporate periods of fasting on most days. It is important to remember however that our weight is not determined by whether we have 10 smaller meals (grazers) or 1-2 much larger meals. Our weight is determined by our caloric intake compared to our energy expenditure.
When my weight was under 60kg I had a body mass index (BMI) less than 22. I felt that I had reached the summit of Mount Everest. Sadly, since 2018, I started to climb down the mountain. I was only under 60kg for 3 weeks in April 2018 and it has been a tough battle since.
I am disappointed that my weight has increased over the last few years and I, like many, have eaten too much sugar and carbohydrate as a way of dealing with the stresses of the COVID-19 pandemic. I am currently 69 kg. I know now is the time for me to again climb to the summit of Mount Everest and follow the advice that I give to my patients. I have been humbled and proud to see so many of my patients achieve their weight loss goals. I will now use my patients as my inspiration. I understand for me weight control is a lifetime battle. I am after all a ‘sugar addict’. The path will not be easy, but I am prepared for the battle ahead.
Dr Christopher Allada
Interventional Cardiologist
Further copies of our article can be found on our website:
https://canberraheart.com.au/wp-content/uploads/2023/03/Understanding_Carbohydrate_Addiction_is_the_Key_to_Weight_Loss.pdf